Liver Disease: An Unseen Threat in Type 2 Diabetes
Introduction
With 420 million diabetics globally (WHO) and India home to 101 million (ICMR, 2023), a parallel silent crisis is emerging: up to 70% of T2D patients develop MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease), yet it goes undiagnosed until irreversible stages. A Lancet study of 30,000+ adults confirms undiagnosed liver fibrosis is common — T2D patients face double the risk of advanced liver scarring versus non-diabetics.
"The liver has high functional reserve and lacks pain receptors — symptoms appear only when significant damage has already occurred." — Dr. Vaibhav Patil, Hepatologist, Rela Hospital
| Statistic | Data |
|---|---|
| Global diabetics | 420 million+ (WHO) |
| India's diabetics | ~101 million (ICMR 2023) |
| T2D patients with MASLD | Up to 70% |
| T2D patients with asymptomatic fibrosis | ~35% |
| Fatty liver's share of fibrosis cases | >90% |
Background & Context
- MASLD (formerly NAFLD/NASH): new nomenclature (2023) reflecting metabolic root cause.
- South Asian genetic predisposition: higher visceral fat at lower BMI → elevated MASLD risk even in non-obese Indians.
- Lancet study (30,000+ adults): strong links between fibrosis, obesity, T2D, and alcohol use.
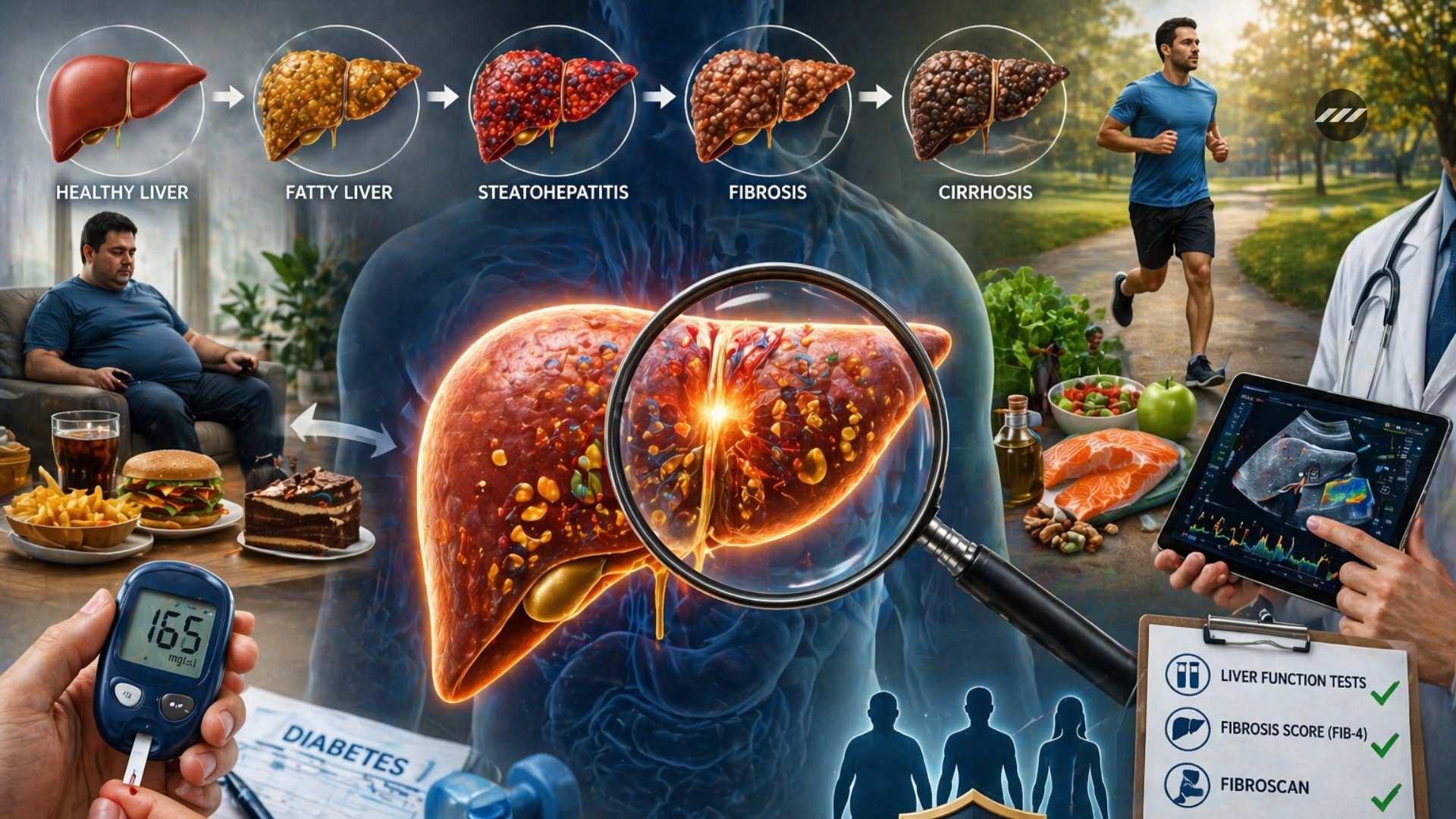
- Disease trajectory: Fat accumulation → Inflammation → Fibrosis → Cirrhosis → Liver cancer — only the first two stages are reversible.
Key Concepts
MASLD Disease Spectrum
| Stage | Condition | Reversibility |
|---|---|---|
| 1 | Hepatic Steatosis (fat accumulation) | Reversible |
| 2 | Steatohepatitis (fat + inflammation) | May regress |
| 3 | Fibrosis (scarring) | Largely irreversible |
| 4 | Cirrhosis (extensive scarring) | Irreversible |
| 5 | Hepatocellular Carcinoma (liver cancer) | Point of no return |
Insulin Resistance — Central Mechanism
T2D → insulin resistance → fat deposited in liver cells → inflammatory cells attracted → chronic inflammation → lipotoxicity (high free fatty acids) → fibrosis. Co-factors: obesity, dyslipidaemia, hypothyroidism, genetic predisposition, gut microbiota disturbance.
Lean NASH — India-Specific Concern
Fatty liver in non-overweight individuals — disproportionately prevalent in South Asia due to visceral fat deposition despite normal BMI. BMI-based screening misses this group entirely; metabolic markers are essential.
Why It Goes Undetected
The liver has high functional reserve and no pain receptors — damage accumulates silently. Symptoms (fatigue, jaundice, abdominal swelling) appear only at advanced stages. Result: 35% of T2D patients have fibrosis with zero symptoms.
Causes of Liver Fibrosis: Beyond Diabetes
| Cause | Mechanism |
|---|---|
| MASLD (metabolic) | Insulin resistance, lipotoxicity, visceral fat |
| Harmful alcohol use | Direct hepatotoxicity; accelerates MASLD |
| Viral hepatitis B & C | Viral inflammation → fibrosis |
| Drug-induced injury | Methotrexate, amiodarone |
| Genetic conditions | Wilson disease (copper), Haemochromatosis (iron) |
Screening Pathway
Step 1 → Liver Function Tests (LFTs): ALT/AST elevation signals injury
[Limitation: may be normal even in significant fibrosis]
Step 2 → FIB-4 Score (Age + AST + ALT + Platelet count):
<1.3 = low risk | >2.67 = high risk → proceed to FibroScan
[Inexpensive, non-invasive, scalable to primary care]
Step 3 → FibroScan (Transient Elastography):
Measures liver stiffness (fibrosis) + CAP score (fat content)
Step 4 → Liver Biopsy: Gold standard; invasive; only if inconclusive
Key principle: Integrate FIB-4 screening into routine diabetes care at primary health level — not only at tertiary centres.
Treatment & Management
| Intervention | Stage | Effect |
|---|---|---|
| Strict glycaemic control | Steatosis / early fibrosis | Reduces fat + inflammation |
| Weight loss (5–10%) | Steatosis / steatohepatitis | Can reverse early MASLD |
| Pioglitazone | Steatohepatitis | Reduces inflammation + fibrosis markers |
| GLP-1 agonists (Semaglutide) | Steatohepatitis / fibrosis | Weight loss + anti-inflammatory liver effect |
| Lipid + alcohol management | All stages | Removes co-damage factors |
| Liver transplant | Cirrhosis / failure | Last resort |
Public Health & Policy Implications
- Lean NASH blind spot: India's BMI-based screening misses high-risk non-obese South Asians — WHO-recommended India-specific cutoff (23 kg/m²) is inconsistently applied.
- Access gap: FibroScan concentrated in tertiary urban centres; FIB-4 (routine blood test) is immediately scalable to primary care.
- Affordability: GLP-1 agonists (semaglutide) are prohibitively expensive — generic access and Ayushman Bharat coverage are policy imperatives.
- Multimorbidity: T2D + MASLD + cardiovascular disease coexist — siloed healthcare delivery fails this patient group; integrated NCD protocols needed under NHM.
Conclusion
MASLD in T2D is a silent epidemic within an epidemic — invisible until irreversible, preventable if caught early. India's 101 million diabetics are a high-risk population requiring mandatory liver screening. The fix is structurally simple: FIB-4 at every diabetes review, FibroScan for high-risk cases, GLP-1 access at affordable prices, and liver health integrated into NHM and Ayushman Bharat protocols. Early screening is not a luxury — it is the difference between reversibility and transplantation.
Attribution
Original content sources and authors
Syllabus classification
How this article maps to GS papers
Main syllabus
GS2HealthcareQuick Q&A
What is the relationship between type 2 diabetes, fatty liver, and liver fibrosis?
However, in a significant proportion of patients, fat deposition triggers chronic inflammation (steatohepatitis), oxidative stress, and lipotoxicity. Over time, this persistent injury leads to the deposition of scar tissue in the liver, known as fibrosis. If fibrosis progresses unchecked, it may culminate in cirrhosis, liver failure, or hepatocellular carcinoma.
The article cites evidence from The Lancet showing that nearly one in three people with diabetes may have silent liver fibrosis. This makes the diabetes-liver disease link not merely a comorbidity but a major public health concern requiring integrated management.
Thus, the progression can be understood as: insulin resistance → fatty liver → inflammation → fibrosis → cirrhosis, with early stages being potentially reversible if detected in time.
Why is liver fibrosis in diabetic patients often called a ‘silent complication’?
Additionally, the liver lacks pain receptors, which means patients do not experience pain or discomfort during the early and intermediate stages of disease progression. Symptoms such as fatigue, jaundice, abdominal swelling, ascites, or fluid retention typically appear only in advanced fibrosis or cirrhosis.
This silent nature makes routine screening essential, especially in high-risk groups like people with T2DM, obesity, dyslipidaemia, and metabolic syndrome. The article highlights that up to 35% of diabetic patients may have fibrosis without symptoms.
The importance lies in the fact that once fibrosis advances to cirrhosis, reversal becomes difficult. Therefore, asymptomatic progression poses a significant challenge to early diagnosis and timely intervention, making it a classic example of a subclinical but high-risk complication.
How does insulin resistance contribute to the progression of liver disease in type 2 diabetes?
These fatty acids are transported to the liver, where they accumulate in hepatocytes, resulting in fatty liver. Excess fat in liver cells causes lipotoxicity, oxidative stress, and recruitment of inflammatory cells. This persistent inflammation leads to hepatocyte injury and activates stellate cells, which produce fibrous scar tissue.
Other associated factors such as obesity, dyslipidaemia, hypothyroidism, and gut microbiota disturbances further worsen this process. Glycated proteins and chronic hyperglycaemia also add to cellular stress.
Therefore, insulin resistance acts as the starting point for a cascade that transforms a metabolic disorder into a progressive liver disease, demonstrating how endocrine dysfunction can directly impact hepatology.
What are the major reasons behind the increasing prevalence of fatty liver and fibrosis among diabetic patients?
Another major factor is the coexistence of other metabolic disorders such as dyslipidaemia, hypertension, and hypothyroidism, which collectively accelerate liver injury. Urbanisation, poor dietary habits, and high-calorie processed food intake further intensify the risk.
The concept of “lean NASH” is also particularly relevant in developing countries like India, where even non-obese individuals may develop fatty liver due to visceral adiposity and genetic predisposition. This challenges the common misconception that only overweight people are at risk.
Additionally, delayed diagnosis due to asymptomatic progression contributes to the apparent increase in prevalence. Improved diagnostic tools such as FibroScan and FIB-4 scoring have also led to better detection rates.
Thus, the issue is multifactorial, involving both lifestyle transitions and biological susceptibility.
Can you explain with an example how routine screening can prevent advanced liver disease in diabetes?
At this stage, timely interventions such as strict glycaemic control, weight reduction, exercise, lipid management, and medications like GLP-1 receptor agonists (e.g., semaglutide) can significantly slow or even halt progression.
Without screening, this patient may remain undiagnosed for years and later present with complications such as cirrhosis, portal hypertension, or liver cancer. This example highlights the value of preventive medicine and early detection.
Hence, routine liver screening in diabetic care functions as a secondary prevention strategy, reducing morbidity, healthcare costs, and long-term mortality.
Critically analyse the need to integrate liver screening into routine diabetes care.
The advantages are significant:
- Early detection of reversible fatty liver
- Risk stratification using FIB-4 and FibroScan
- Timely therapeutic interventions
- Reduction in progression to cirrhosis and cancer
However, challenges include cost, limited availability of non-invasive tools in rural settings, and lack of awareness among both physicians and patients.
From a public health perspective, integrating screening into existing diabetes programmes can improve outcomes substantially. In India, where diabetes prevalence is high, this could be aligned with NCD clinics under the National Health Mission.
Thus, the case for integration is strong, though it must be accompanied by capacity building, affordability, and awareness campaigns.
As a public health administrator, how would you design a screening strategy for liver fibrosis among diabetic patients?
Patients identified as moderate- or high-risk would be referred to secondary or tertiary centres for FibroScan and specialist hepatology consultation. High-risk groups such as obese patients, those with dyslipidaemia, or long-standing diabetes should be prioritised.
Public awareness campaigns would emphasise that fatty liver can occur even in lean individuals. Integration with NPCDCS clinics and digital health records would ensure follow-up and continuity of care.
This strategy combines preventive screening, risk-based referral, and lifestyle intervention, making it suitable for a resource-constrained but high-burden setting like India.
Practice questions
1 question for mains preparation